|
|
Background
One of the primary objectives of maintenance parenteral fluid therapy is to provide water to meet physiologic losses (insensible loss + urine loss). In a study published in 1957, in the Journal Pediatrics, Malcolm Holliday and William Segar developed a simple scheme which could be easily remembered to calculate the maintenance water needs in hospitalized patients.
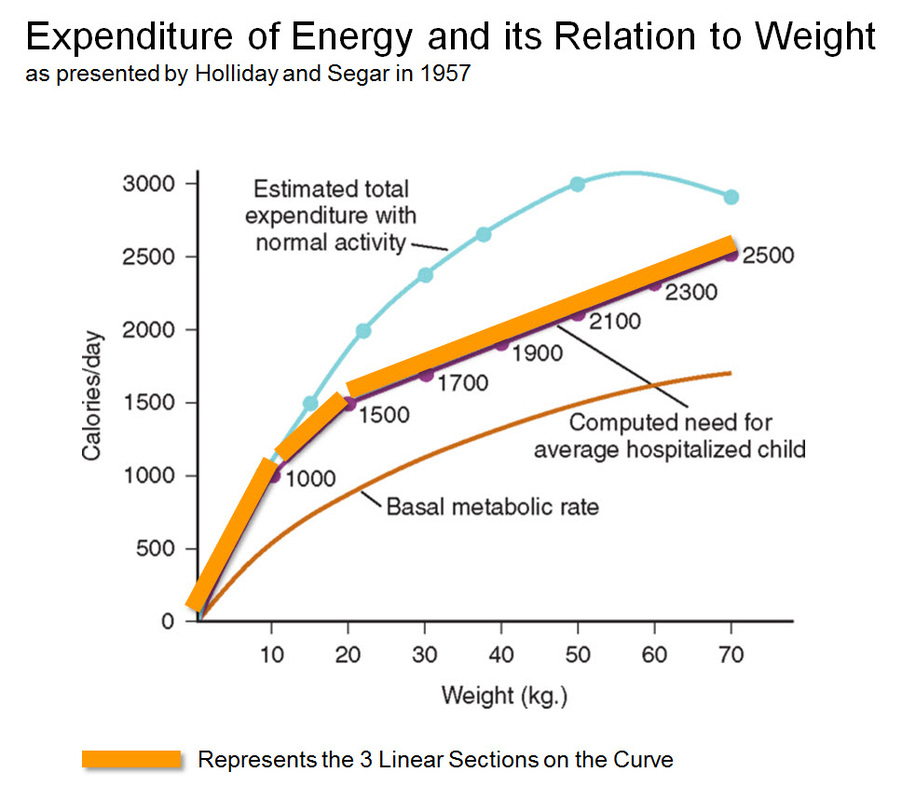
Assimilating the known physiology at the time, they observed that “there was a DIRECT LINEAR relationship between Physiologic Water Needs (insensible losses + urinary losses) and Energy Metabolism". In other words “the average needs for water, expressed in milliliters, equals energy expenditure in calories (under normal resting conditions, 1 ml of water is required to metabolize 1 kcal)".
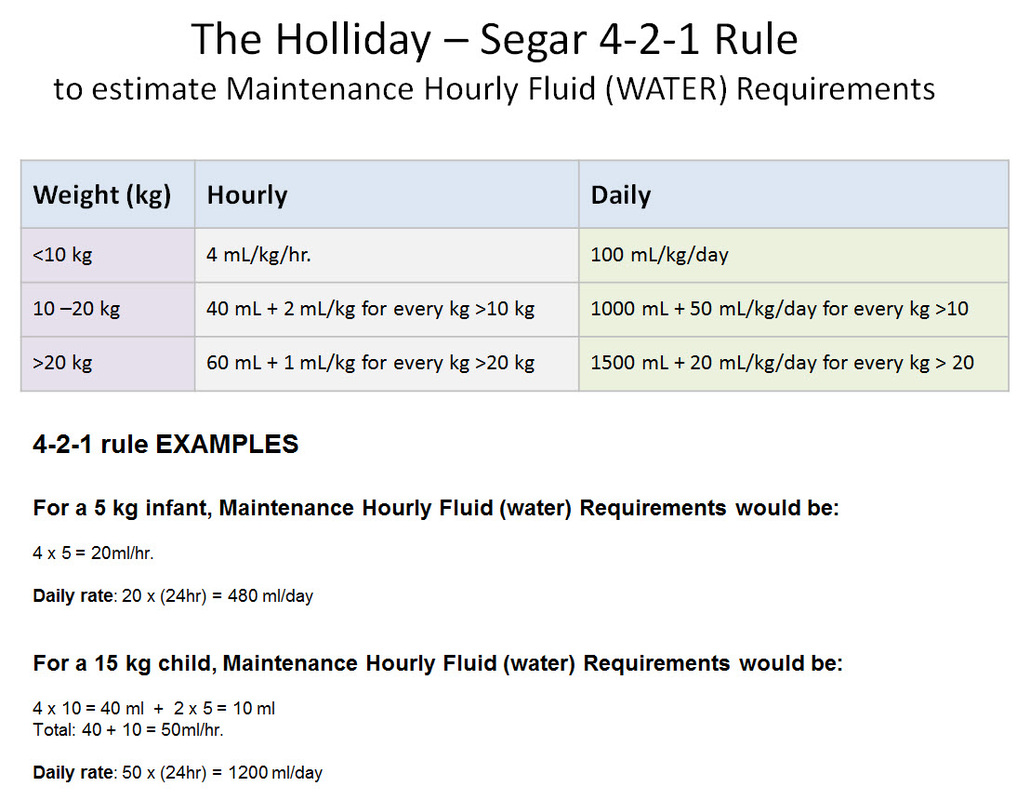
The relationship between Weight and Energy Expenditure was found to be NON-LINEAR. Based on their data and assumptions, Holliday and Segar constructed a curve plotting Energy Caloric Requirements versus Weight. This curve could be seen comprising of three linear sections which coincided approximately with the following weight sections: 0 to 10 kg, 10 to 20 kg, and 20 to 70 kg. Viewed in this manner, the authors concluded that 100 mL/kg/day for weights to 10 kg, an additional 50 mL/kg/day for each kilogram from 11 to 20 kg, and 20 mL/kg/day more for each kilogram beyond 20 kg. In anesthetic practice, this formula has been further simplified, with the hourly requirement referred to as the “4-2-1 rule” (4 mL/kg/hr for the first 10 kg of weight, 2 mL/kg/hr for the next 10 kg, and 1 mL/kg/hr for each kilogram thereafter.
Assimilating the known physiology at the time, they observed that “there was a DIRECT LINEAR relationship between Physiologic Water Needs (insensible losses + urinary losses) and Energy Metabolism". In other words “the average needs for water, expressed in milliliters, equals energy expenditure in calories (under normal resting conditions, 1 ml of water is required to metabolize 1 kcal)".
The relationship between Weight and Energy Expenditure was found to be NON-LINEAR. Based on their data and assumptions, Holliday and Segar constructed a curve plotting Energy Caloric Requirements versus Weight. This curve could be seen comprising of three linear sections which coincided approximately with the following weight sections: 0 to 10 kg, 10 to 20 kg, and 20 to 70 kg. Viewed in this manner, the authors concluded that 100 mL/kg/day for weights to 10 kg, an additional 50 mL/kg/day for each kilogram from 11 to 20 kg, and 20 mL/kg/day more for each kilogram beyond 20 kg. In anesthetic practice, this formula has been further simplified, with the hourly requirement referred to as the “4-2-1 rule” (4 mL/kg/hr for the first 10 kg of weight, 2 mL/kg/hr for the next 10 kg, and 1 mL/kg/hr for each kilogram thereafter.