|
|
Positioning Infants and Children for Airway Management
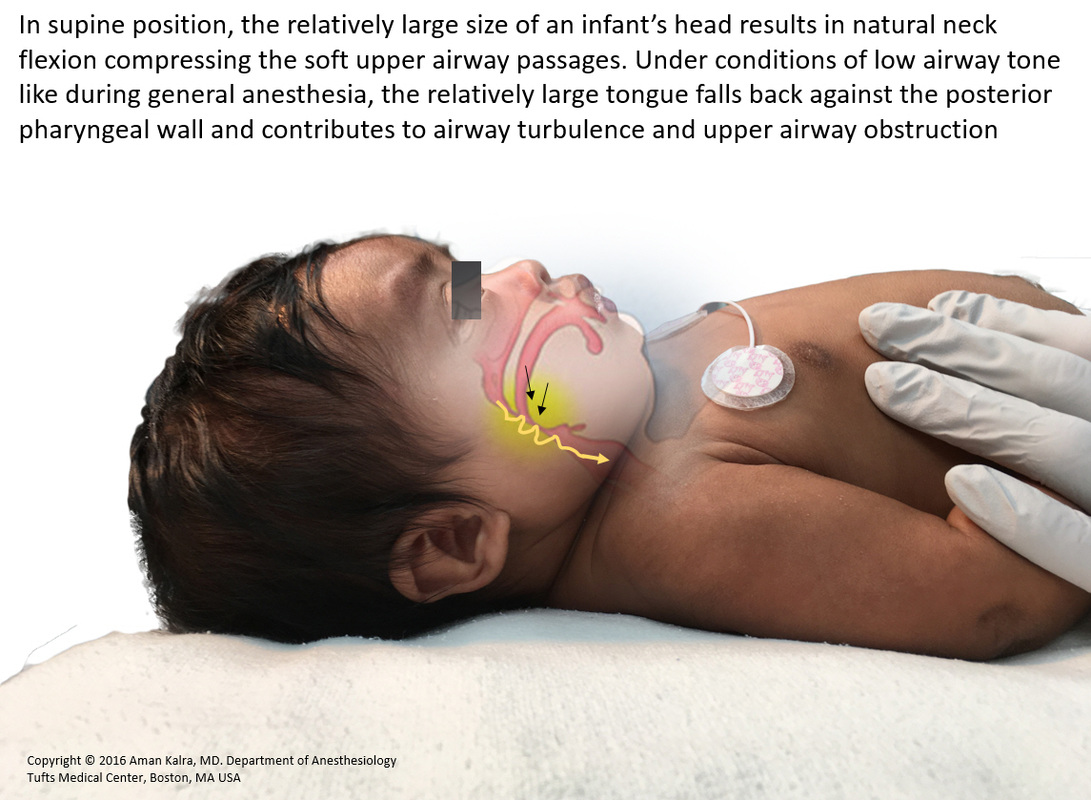
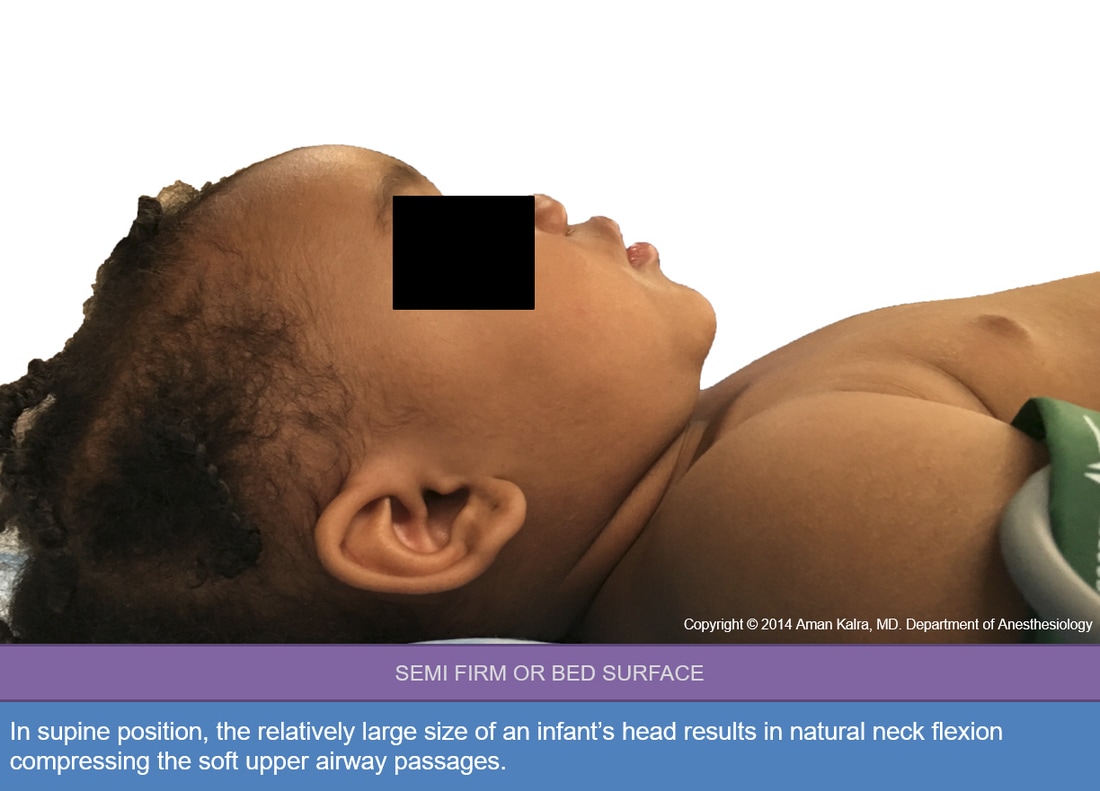
In supine position, the relatively large size of an infant’s head results in natural neck flexion compressing the soft upper airway passages. Under conditions of low airway tone like during general anesthesia, the relatively large tongue falls back against the posterior pharyngeal wall and contributes to airway turbulence and upper airway obstruction.
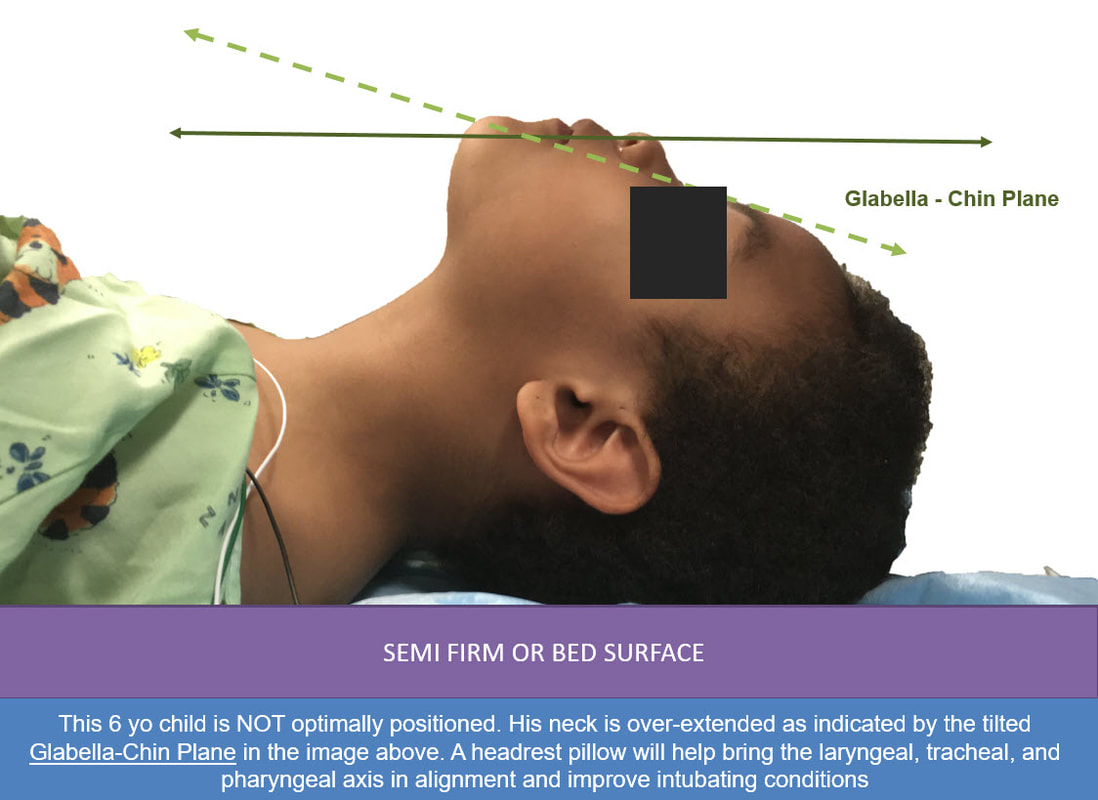
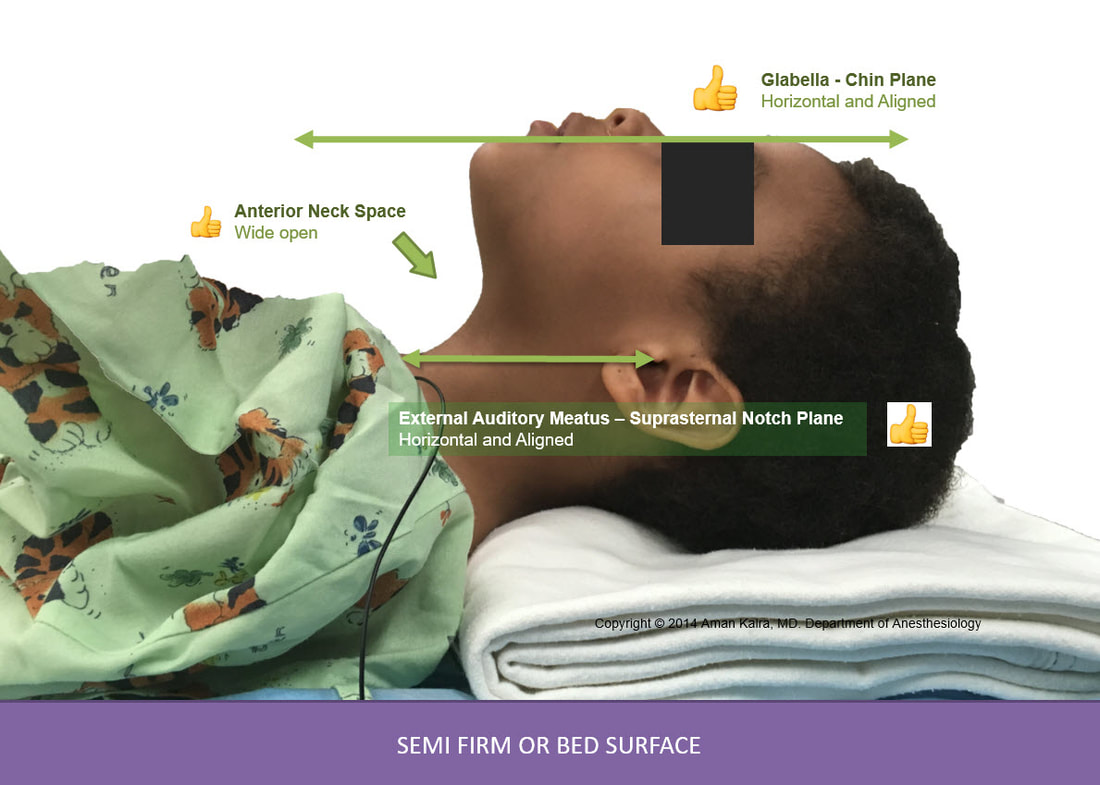
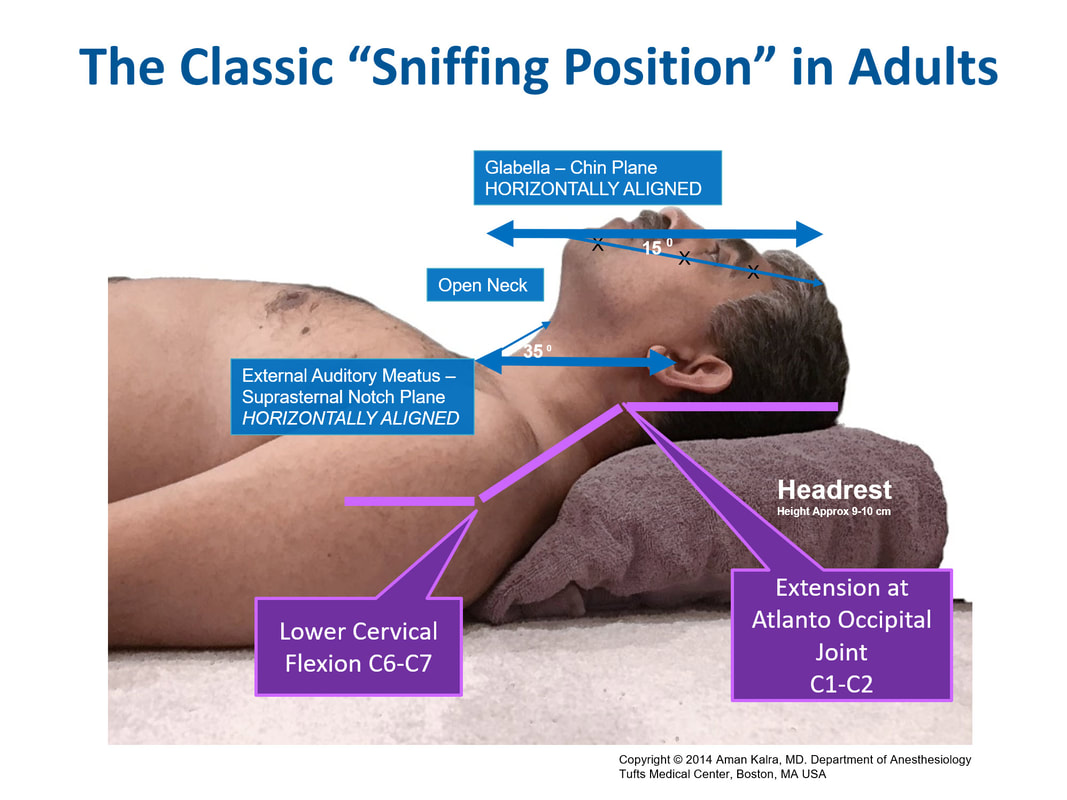
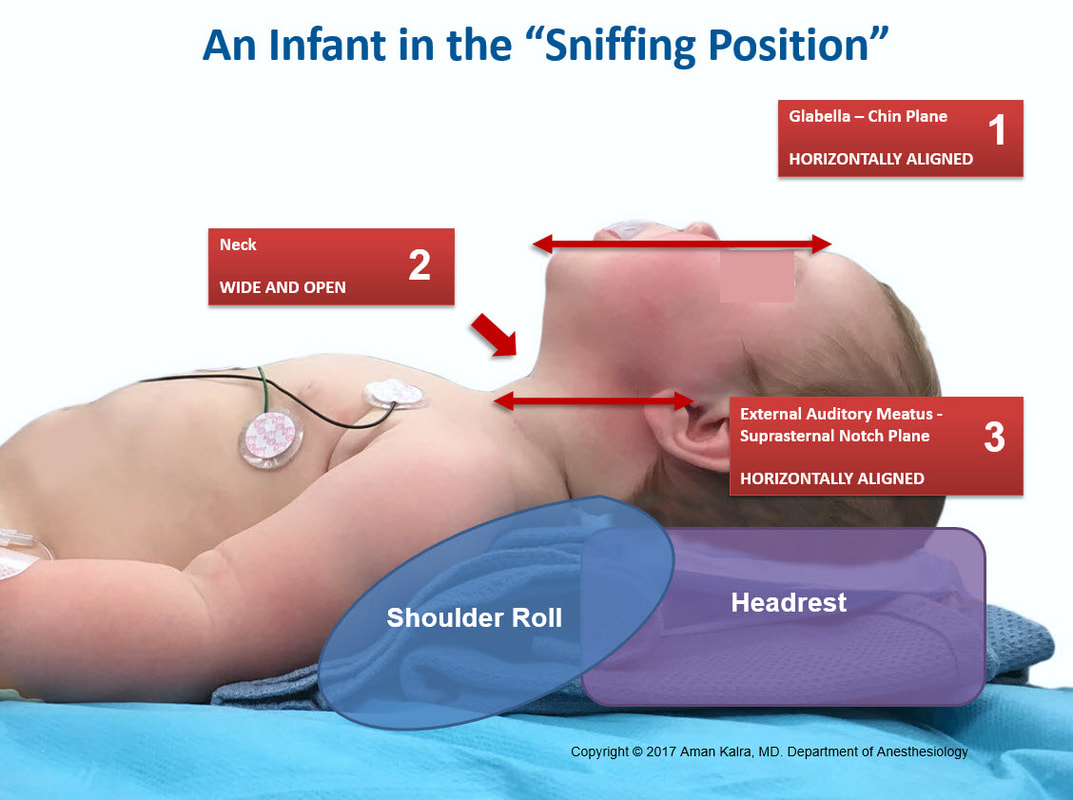
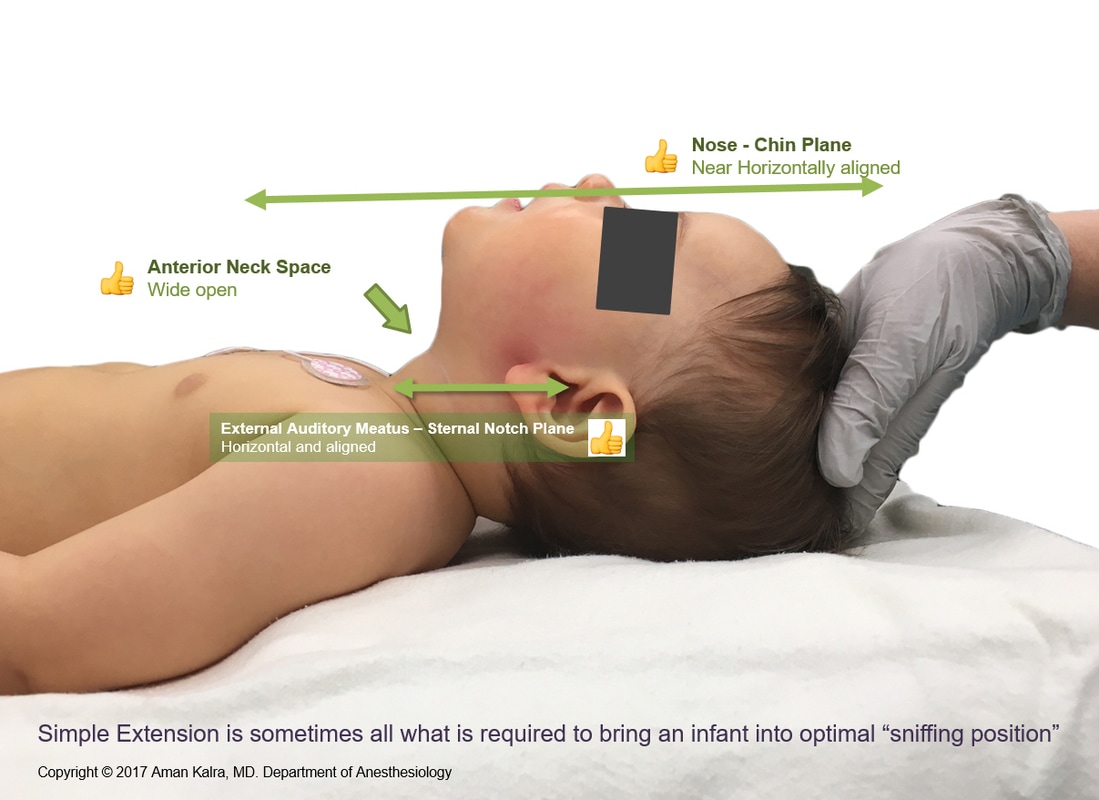
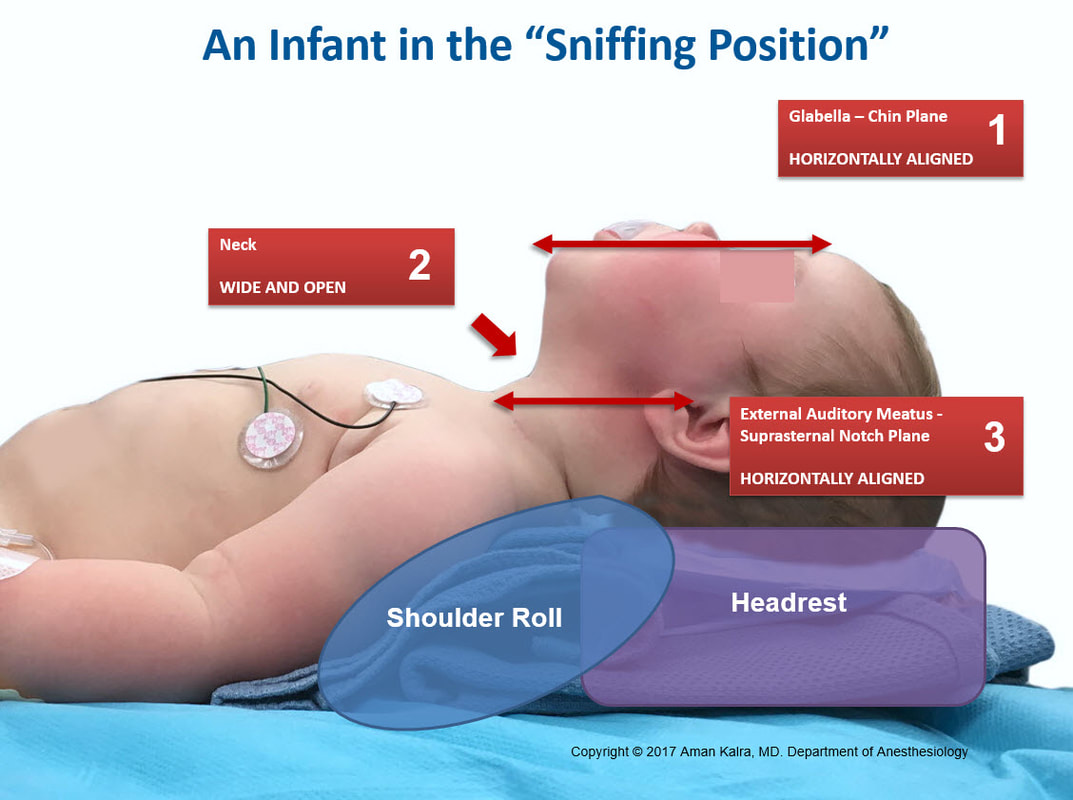
The classic sniffing position is an established standard across anesthesia practice. Simple extension of the neck can bring an infant into optimal sniffing position. More often than not, a combination of a shoulder roll and head rest is required as shown in the graphics below. Notice, how the Glabella - Chin Plane is near horizontal to the ceiling, and the neck is wide open. The External Auditory Meatus (EAM) is also observed to be in horizontal alignment with the Suprasternal notch (SN). These 3 visual markers can facilitate us to position children in the sniffing position. Neck over-extension must be avoided as it can make laryngeal exposure difficult.
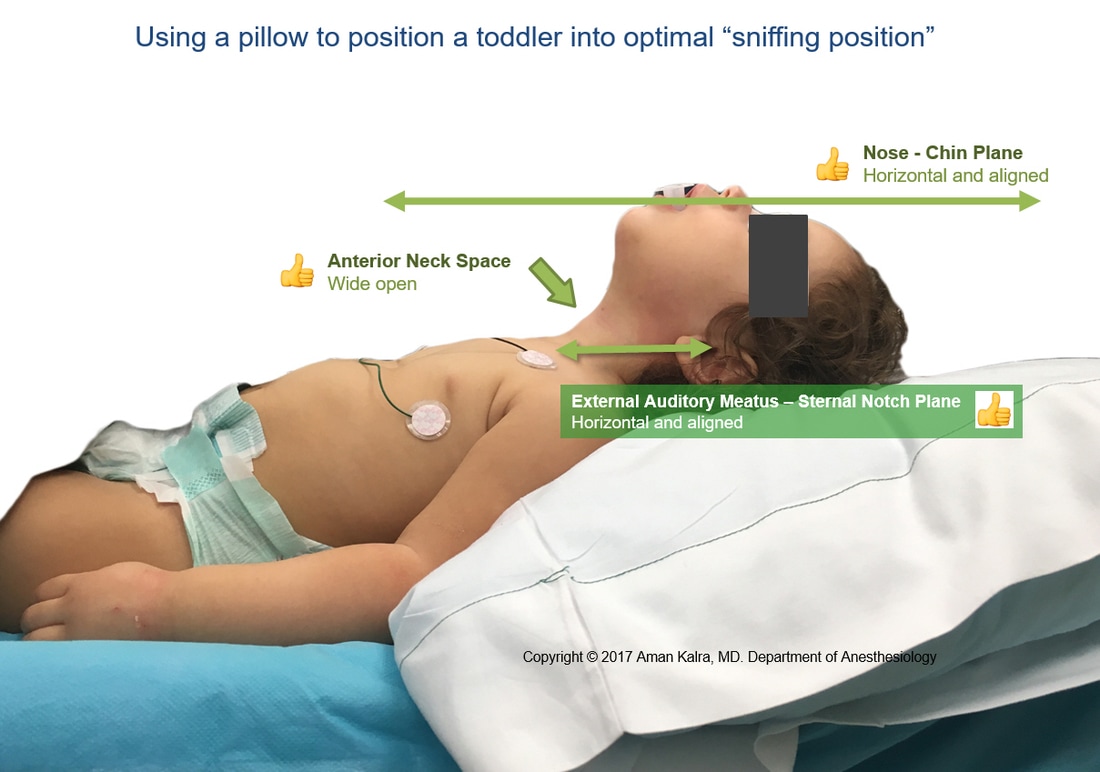
When positioning older children, a head rest is generally sufficient to bring patients in optimal sniffing position. The principles governing obese children are similar to that of adults.
The classic sniffing position is an established standard across anesthesia practice. Simple extension of the neck can bring an infant into optimal sniffing position. More often than not, a combination of a shoulder roll and head rest is required as shown in the graphics below. Notice, how the Glabella - Chin Plane is near horizontal to the ceiling, and the neck is wide open. The External Auditory Meatus (EAM) is also observed to be in horizontal alignment with the Suprasternal notch (SN). These 3 visual markers can facilitate us to position children in the sniffing position. Neck over-extension must be avoided as it can make laryngeal exposure difficult.
When positioning older children, a head rest is generally sufficient to bring patients in optimal sniffing position. The principles governing obese children are similar to that of adults.
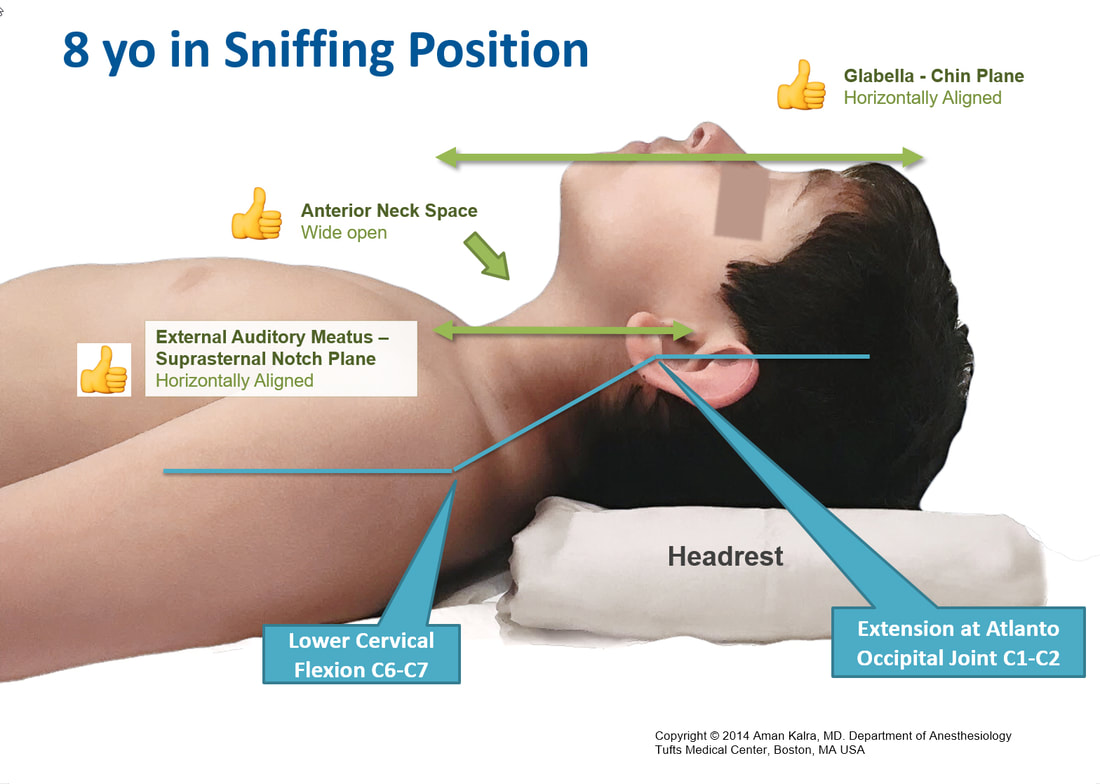
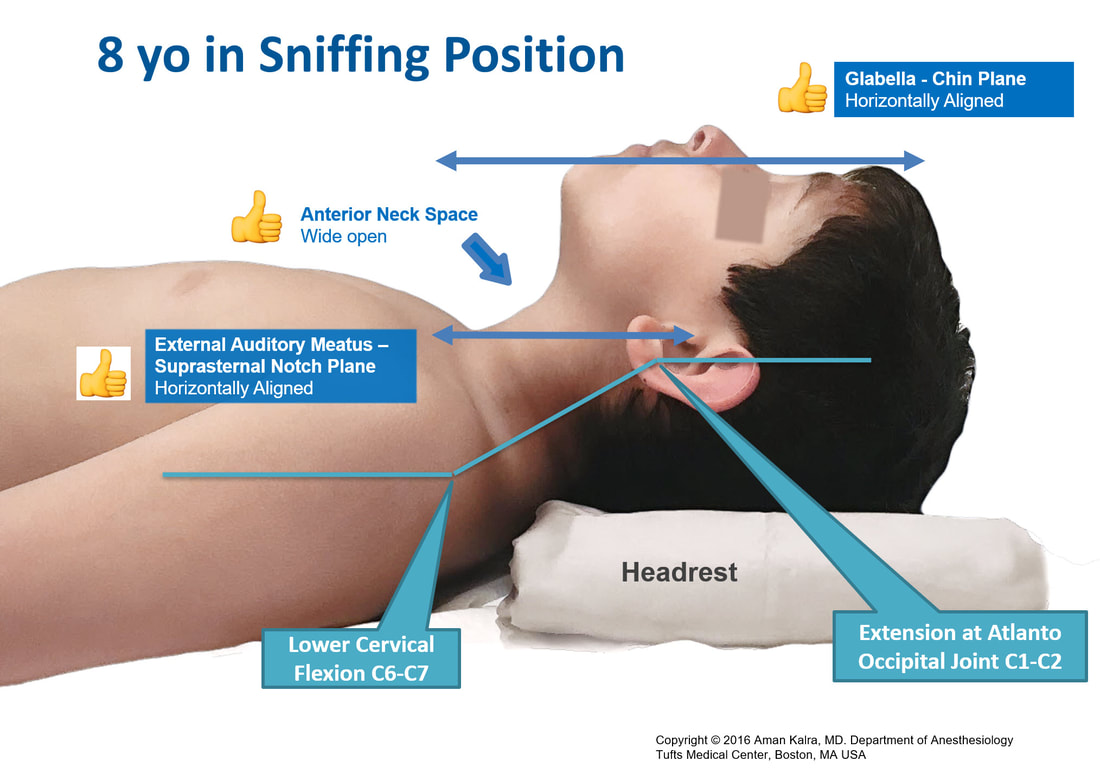
The above principles can easily be extended to older children and adolescents as is evidenced by the image below
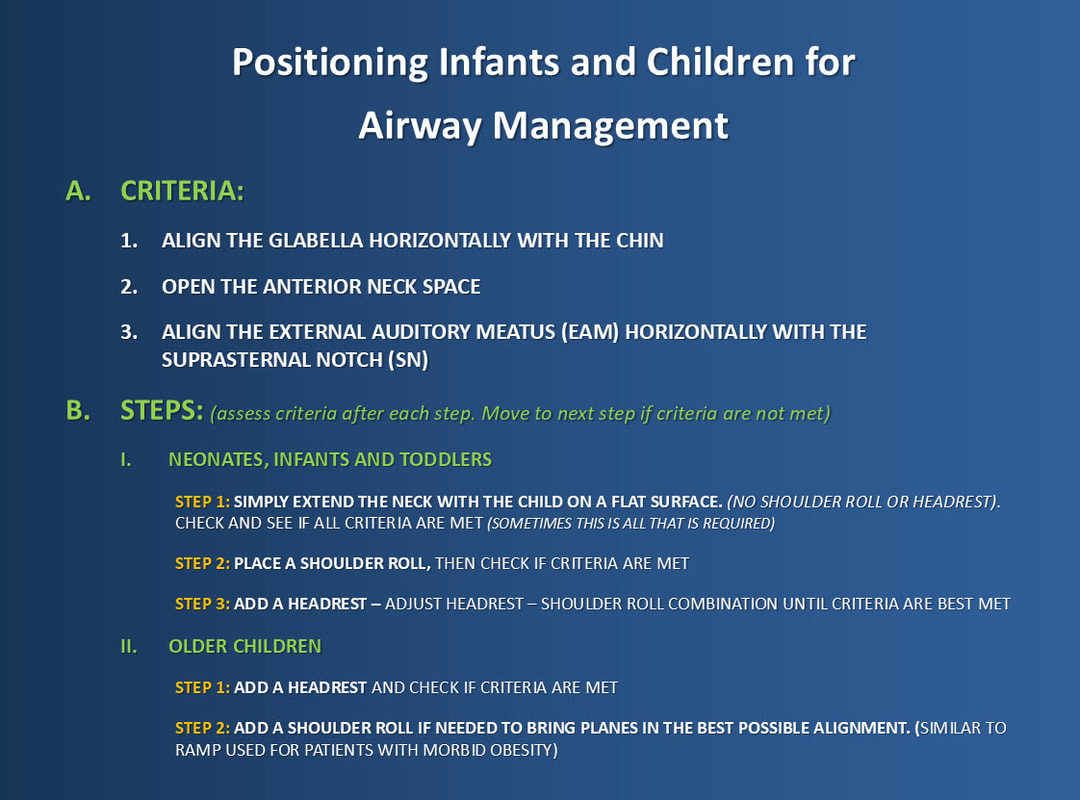
Positioning Infants and Toddlers correctly requires a step wise approach is detailed below:
|
|
NEONATES, INFANTS AND TODDLERS
STEP 1: SIMPLE EXTENSION
(No Shoulder Roll or Headrest)
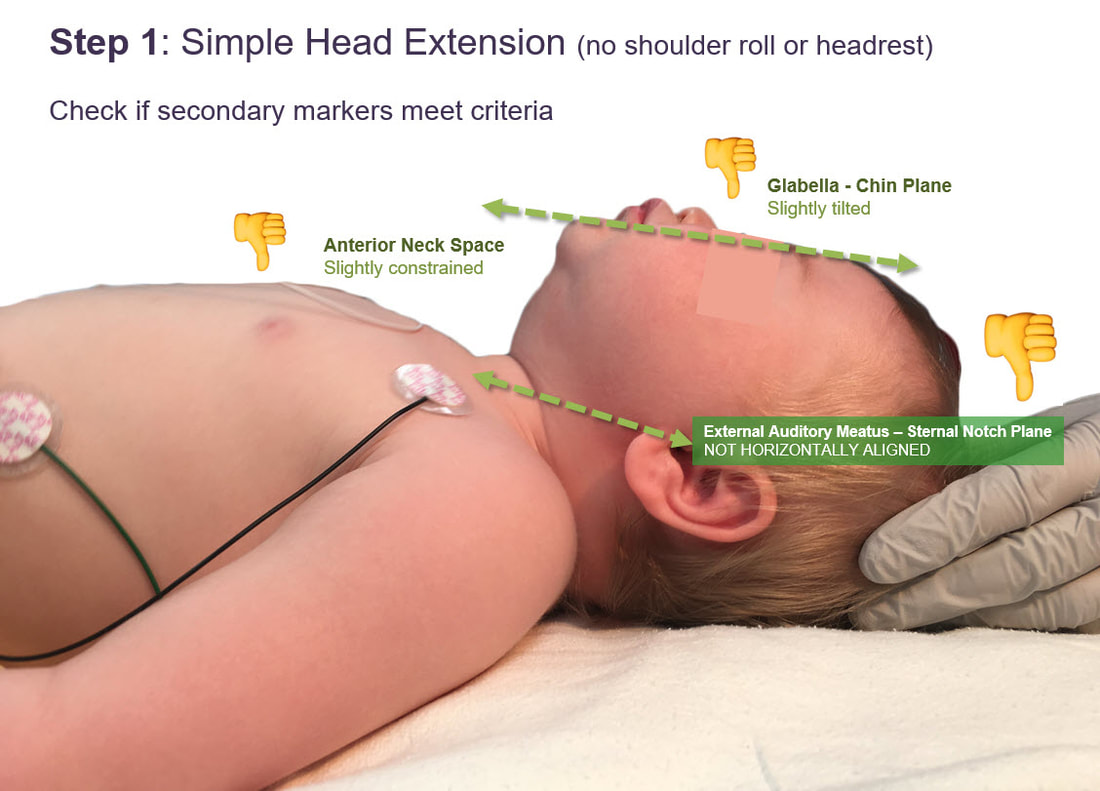
In the above example, simple head extension is not bringing the EAM-SN plane in horizontal alignment. However, some cases, simple extension will suffice and bring the planes in alignment as is seen in the two examples below
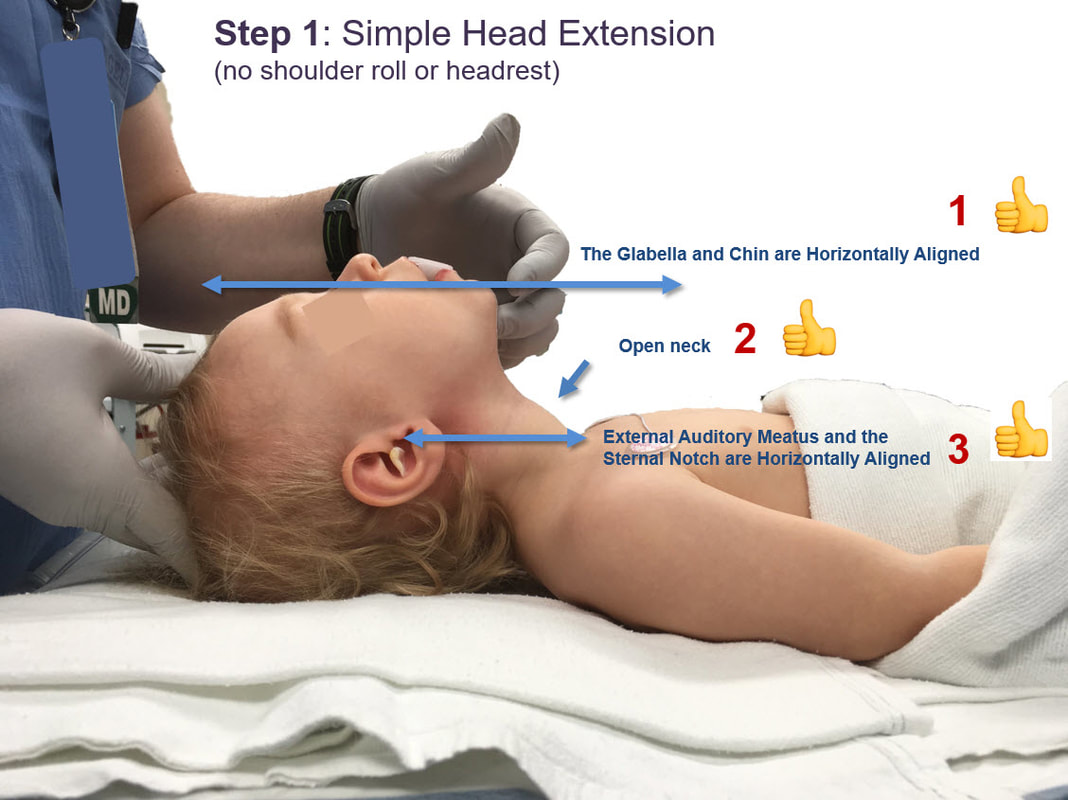
CLINICAL PEARL: SIMPLE HEAD EXTENSION MAY BRING SOME INFANTS IN THE SNIFFING POSITION.
If Step 1 fails to bring the planes in horizontal alignment, proceed to Step 2 and 3
NEONATES, INFANTS AND TODDLERS
STEP 2: PLACE A SHOULDER ROLL
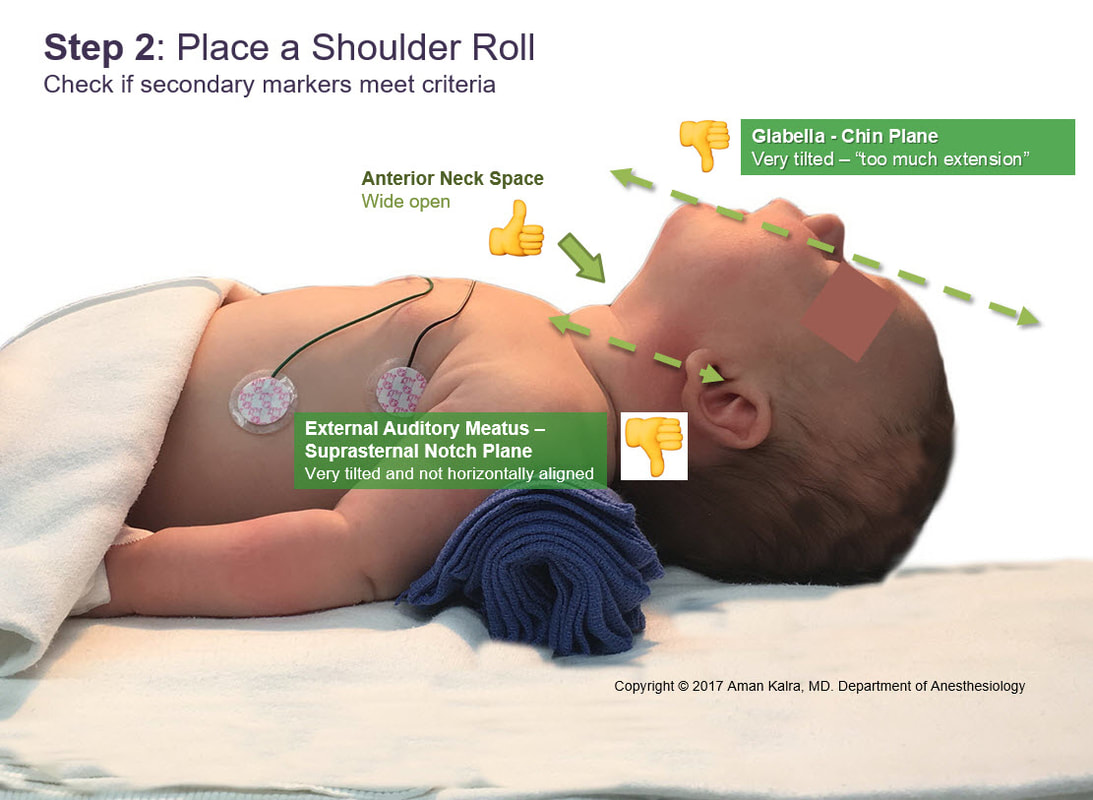
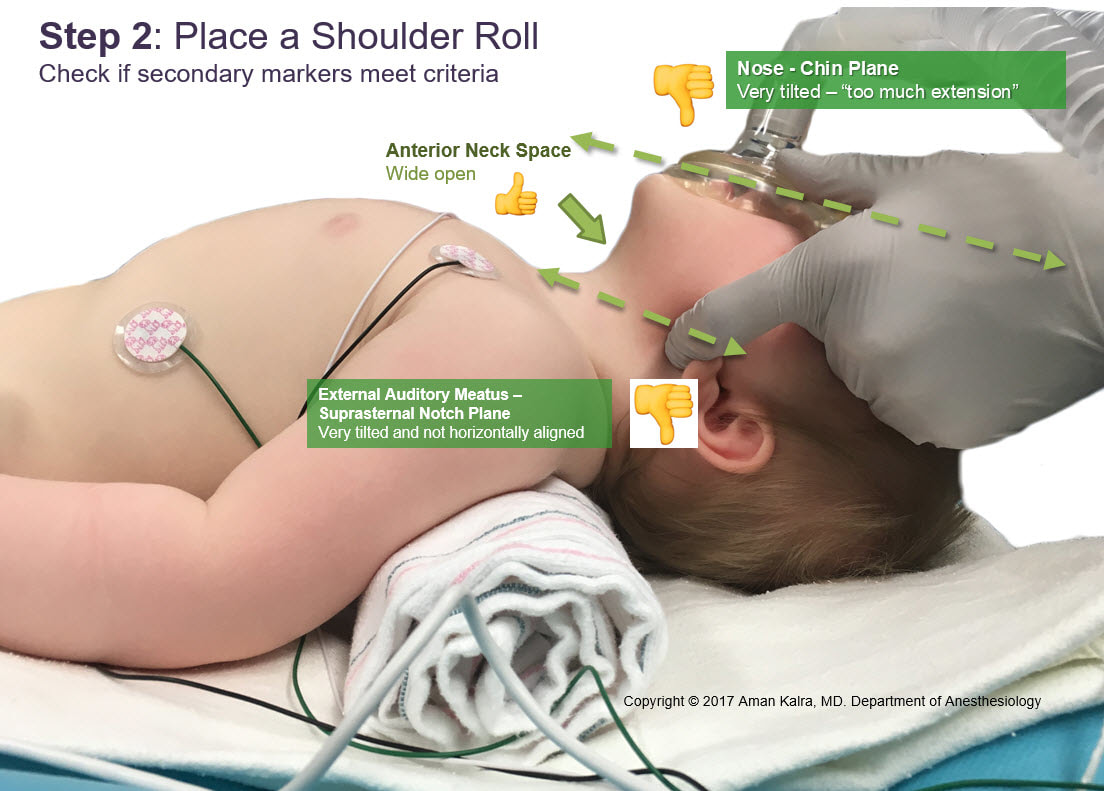
Generally a shoulder roll will tend to hyperextend the head, and a balancing headrest is necessary to horizontally align the planes
NEONATES, INFANTS AND TODDLERS
STEP 3: ADD A HEADREST
(Shoulder Roll adjustment may be required)

OLDER CHILDREN
STEP 1: ADD A HEADREST
(Shoulder Roll Combo may be required in Obese Children)