
|
|
|
|
|
|
OR SETUP - STEP 4
Prepare the OR Table and Positioning Props
A. Prepare the OR Table
For neonates, infants, and children, a Baer Hugger / Mistral Air Forced Air Warming Underbody Blanket should be placed securely on the OR bed. These come in two sizes - Neonate Plus and Large Pediatric Underbody. For older children and young adults, a regular upper or lower body Baer Hugger blanket should be considered.
The size of the operating bed may have to altered for neonates and infants. Communicate with your Attending Pediatric Anesthesiologist before making any alterations.
The size of the operating bed may have to altered for neonates and infants. Communicate with your Attending Pediatric Anesthesiologist before making any alterations.
B. Positioning Props
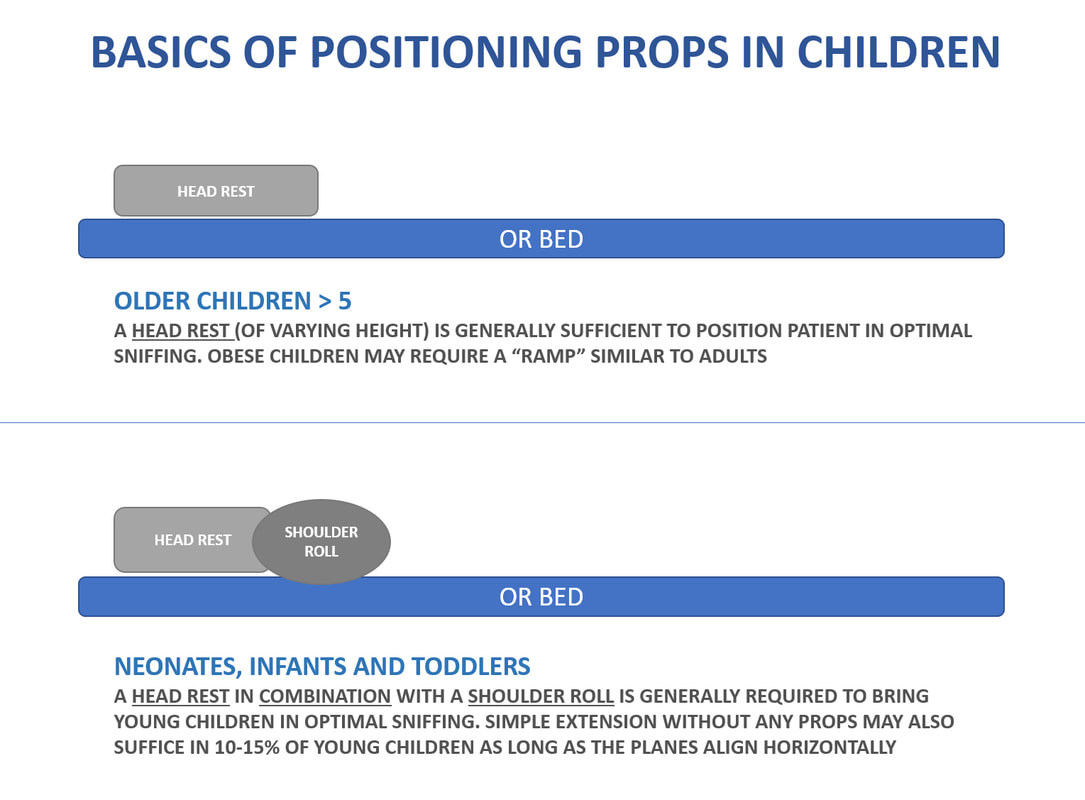
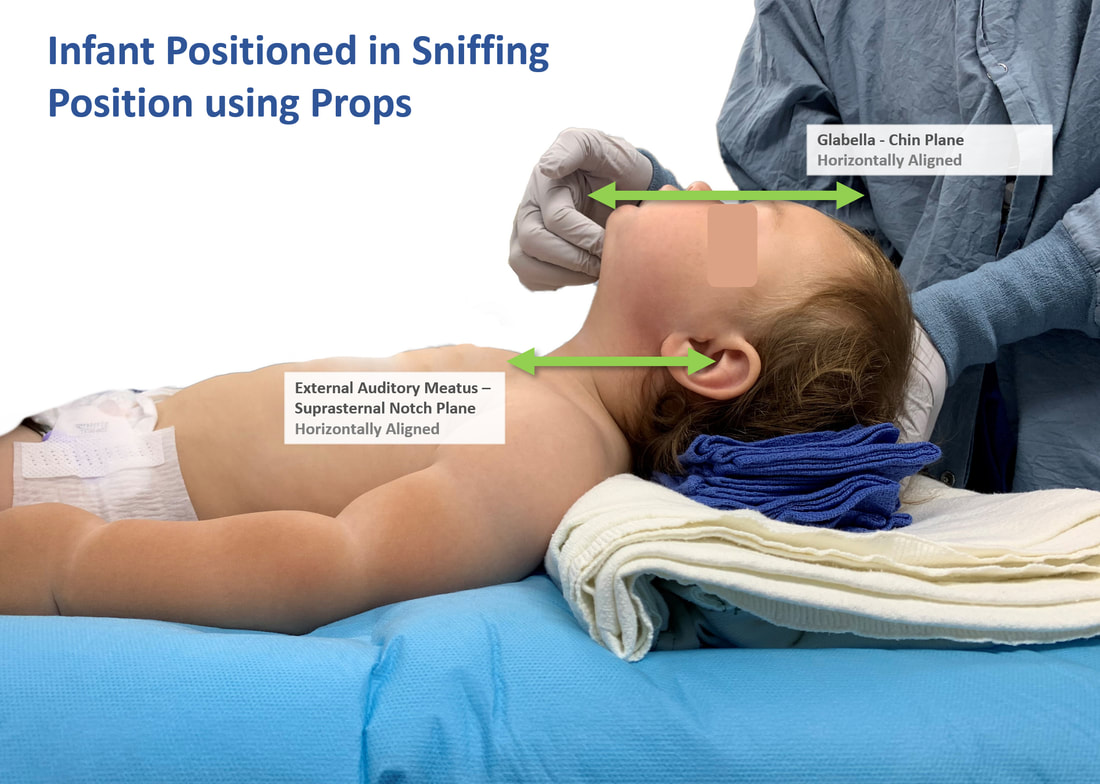
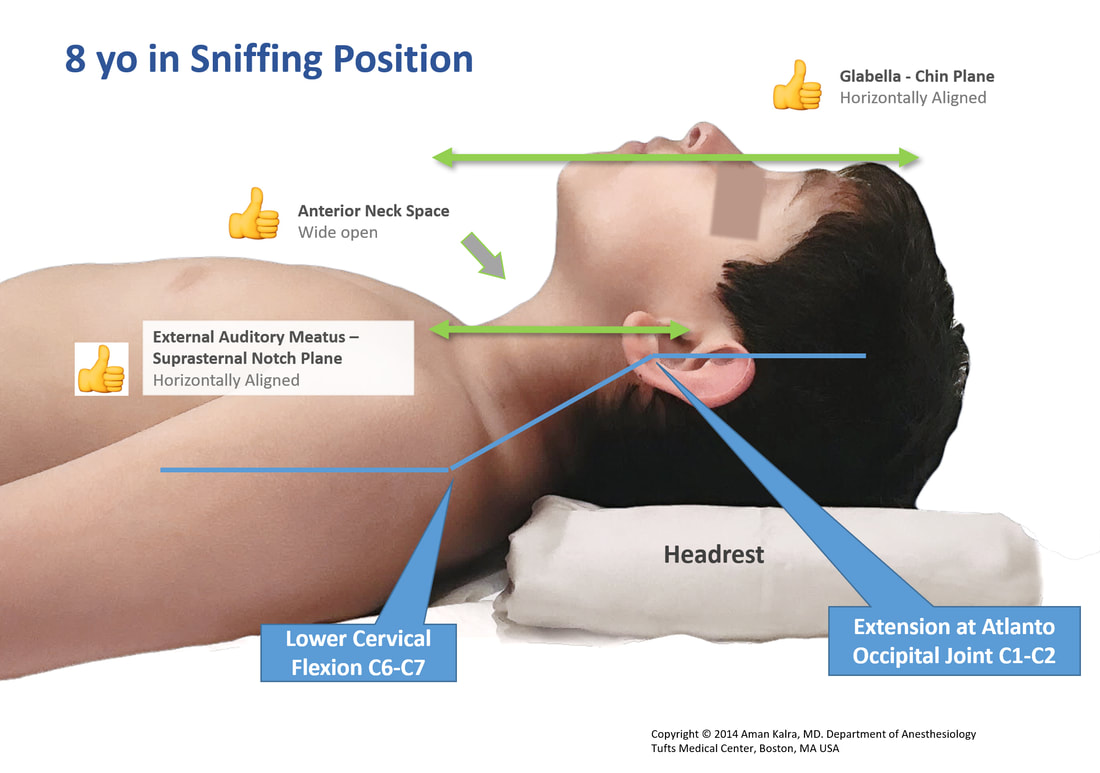
The classic sniffing position is an established standard across anesthesia practice. To bring children in the most optimal sniffing position, we must aim to align the External Auditory Meatus (EAM) in horizontal plane with the Suprasternal notch (SN). The Glabella - Chin face plane should also be near horizontal.
In older children, a head rest (of variable height depending on size of patient) is generally sufficient to achieve optimal sniffing. Older obese children may require ramping similar to practice in adults.
In infants and toddlers, a shoulder roll in combination with a head rest is recommended to optimally position for airway management. In a small proportion of infants and toddlers, simple head extension without any props may be sufficient to bring the planes in horizontal alignment.
Props can be created using different techniques and materials. the images below will demonstrate various common combinations.
In older children, a head rest (of variable height depending on size of patient) is generally sufficient to achieve optimal sniffing. Older obese children may require ramping similar to practice in adults.
In infants and toddlers, a shoulder roll in combination with a head rest is recommended to optimally position for airway management. In a small proportion of infants and toddlers, simple head extension without any props may be sufficient to bring the planes in horizontal alignment.
Props can be created using different techniques and materials. the images below will demonstrate various common combinations.
|
|