|
|
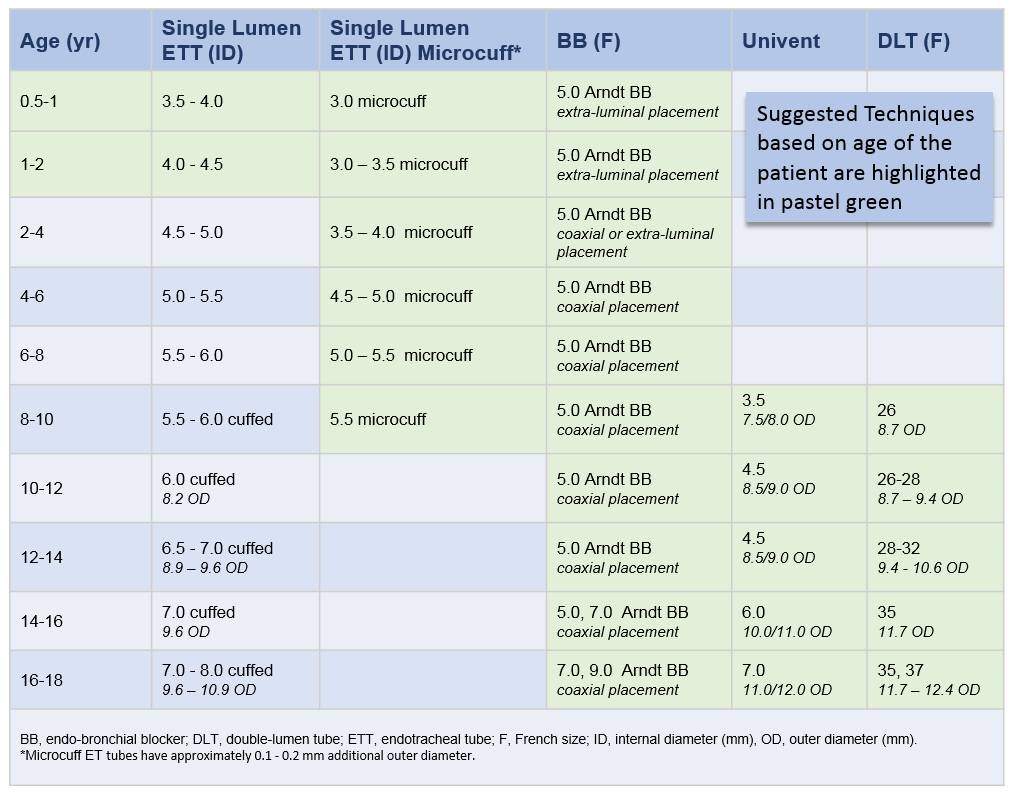
Single-Lumen Endotracheal Tube
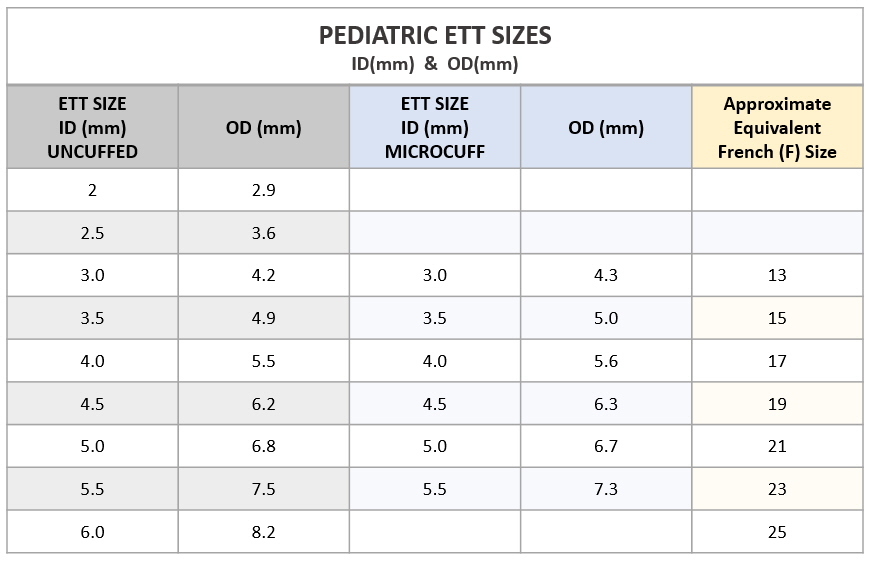
In infants and very small children (3 and under), the easiest means of providing SLV is to intentionally intubate the main stem bronchus of the non-operated lung. A pediatric bronchoscope placed through the ETT is extremely helpful in guiding and confirming accurate placement. This is particularly true when intubating the left main-stem bronchus for right sided thoracotomies. The size of the single-lumen ETT chosen should take into consideration the diameter of the main-stem bronchus and not just the trachea. An uncuffed single-lumen ETT may not provide adequate seal of the bronchus and may prevent satisfactory collapse of the operative lung . In this regard, Kimberly Clark Microcuff ETTs are a great choice. Please do note that the outer diameter (OD) of microcuff ET tubes is 0.1 - 0.2 mm larger than comparable regular uncuffed single lumen ETTs.
Arndt Endobrochial Blocker
The Arndt Endobronchial blocker is intended to deferentially intubate a patient's bronchus in order to isolate the left or right lung for procedures that require one-lung ventilation.
The Pediatric Arndt Endobronchial Blocker is available only in 5F size. ET tubes 4.5 ID and over can easily accommodate a 5F blocker alongside a small diameter flexible fiberoptic bronchoscope. Specialty multiport adapters are included with these kits to facilitate ventilation during placement of the blocker.
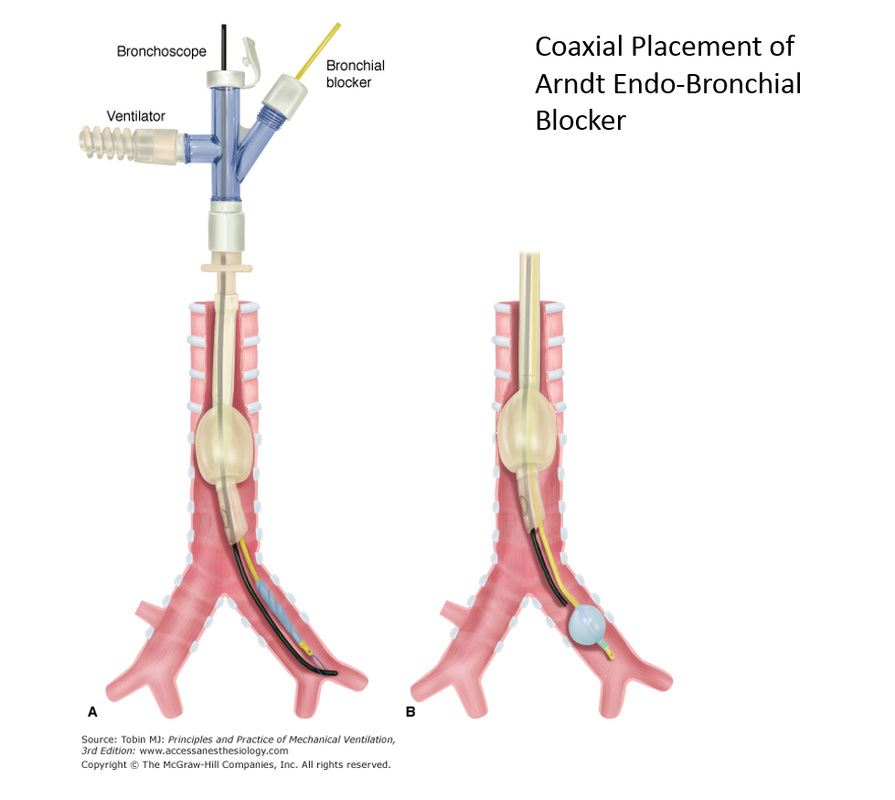
The Arndt Endobronchial blocker can be used in TWO CONFIGURATIONS depending on the age of the patient and the size of the ET tube:
1. The classical coaxial placement through the lumen of the ETT is recommended when using cuffed endotracheal tubes sizes 4.5 ID and over.
2. Parallel extra-luminal placement is recommended when using the arndt endo-bronchial blocker in infants and small children (under 24 months).
Potential Problems with Endobronchial Blockers: One potential problem with this technique is the possibility of dislodgement of the blocker balloon back into the trachea, blocking ventilation to both lungs.
The Pediatric Arndt Endobronchial Blocker is available only in 5F size. ET tubes 4.5 ID and over can easily accommodate a 5F blocker alongside a small diameter flexible fiberoptic bronchoscope. Specialty multiport adapters are included with these kits to facilitate ventilation during placement of the blocker.
The Arndt Endobronchial blocker can be used in TWO CONFIGURATIONS depending on the age of the patient and the size of the ET tube:
1. The classical coaxial placement through the lumen of the ETT is recommended when using cuffed endotracheal tubes sizes 4.5 ID and over.
2. Parallel extra-luminal placement is recommended when using the arndt endo-bronchial blocker in infants and small children (under 24 months).
Potential Problems with Endobronchial Blockers: One potential problem with this technique is the possibility of dislodgement of the blocker balloon back into the trachea, blocking ventilation to both lungs.

Univent Tube (Fuji Systems Corp)
Double Lumen Tubes
Tube Selection for Single Lung Ventilation (SLV) in Infants and Children