|
|
|
|
|
|
OR SETUP - STEP 6
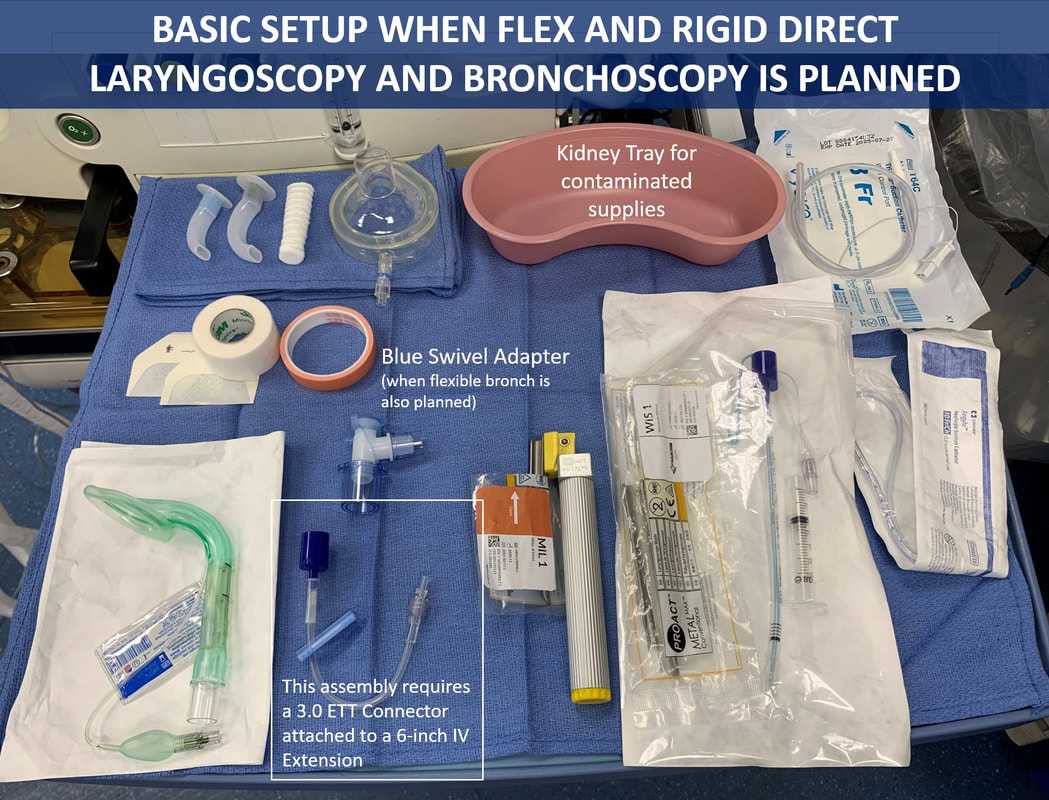
Prepare Airway Desktop
A. Essential Components of a Basic Pediatric Airway Desktop
The image below shows all the components of a Basic Standard Pediatric Airway Desktop. All these supplies must be readily available. Leave Guedel airways, suction catheters, R'pogle NG/OG tubes, extra ETTs in their original packing to prevent wastage and contamination. Only one pediatric handle needs to be out on the desk. The other can stay in the drawer.
These essential supplies are listed below:
These essential supplies are listed below:
- Pedi Laryngoscope Handle
- 2 Pedi Laryngoscope Blades based on age and size of patient (leave secondary blade in package)
- Guedel Oral Airway. Have multiple sizes available. (leave in package)
- Anesthesia Masks (have at least 2 sizes available)
- Microcuff ETTs with 3cc syringes for cuff inflation. Have additional smaller sizes ETTs available (leave in package)
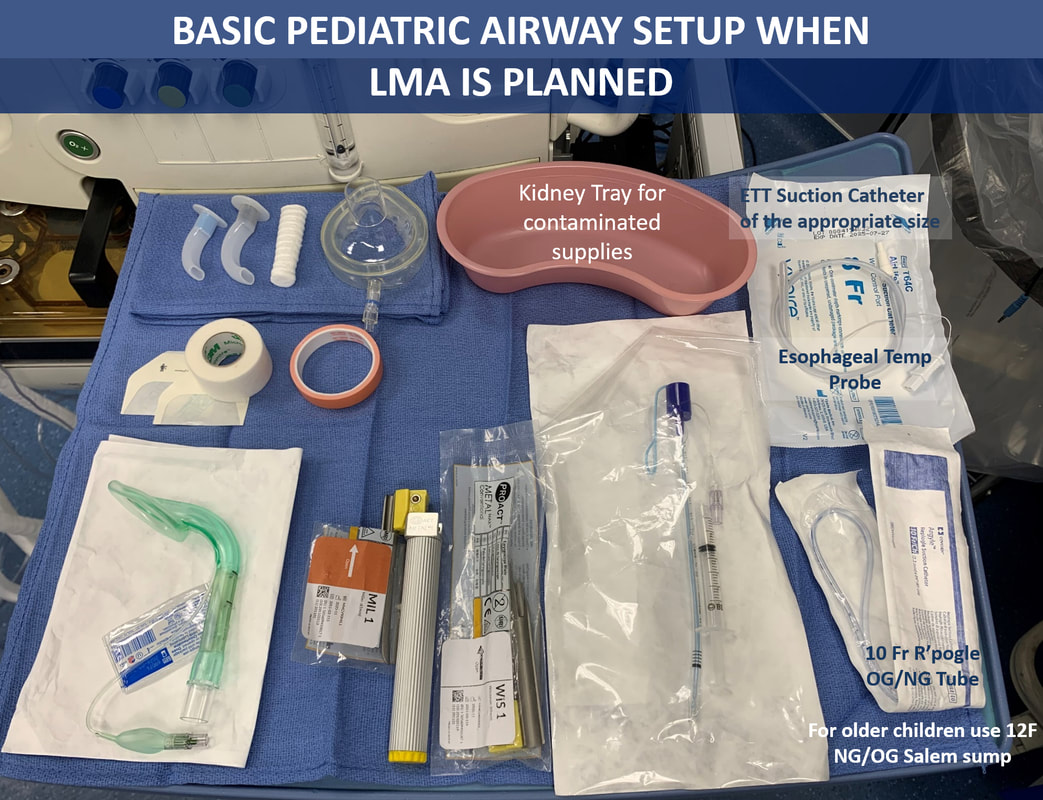
- 10F Repogle NGT (for infants) or 12 Fr OG/NG (older children) for rapid gastric decompression. (leave in package)
- ETT suction catheter of the appropriate size (6, 8. & 10F). Note that only size 6F passes through 3.0 ETT
- Esophageal/Rectal Temp Probe (available in two sizes: 9 and 12F)
- Pink and White Silk tape.
- A Special 3M White Cloth Tape is used to secure ETT when post op intubation is planned.
- Mastisol adhesive. (leave in cart)
- 3M Micropore Paper Tape and Tegaderm x 2
- Pediatric Bite Block. Small and medium sizes available. (leave in package)
- Tongue Depressor (leave in package)
- Kidney Tray for keeping contaminated supplies

B. Examples of Other Basic Pediatric Airway Setups

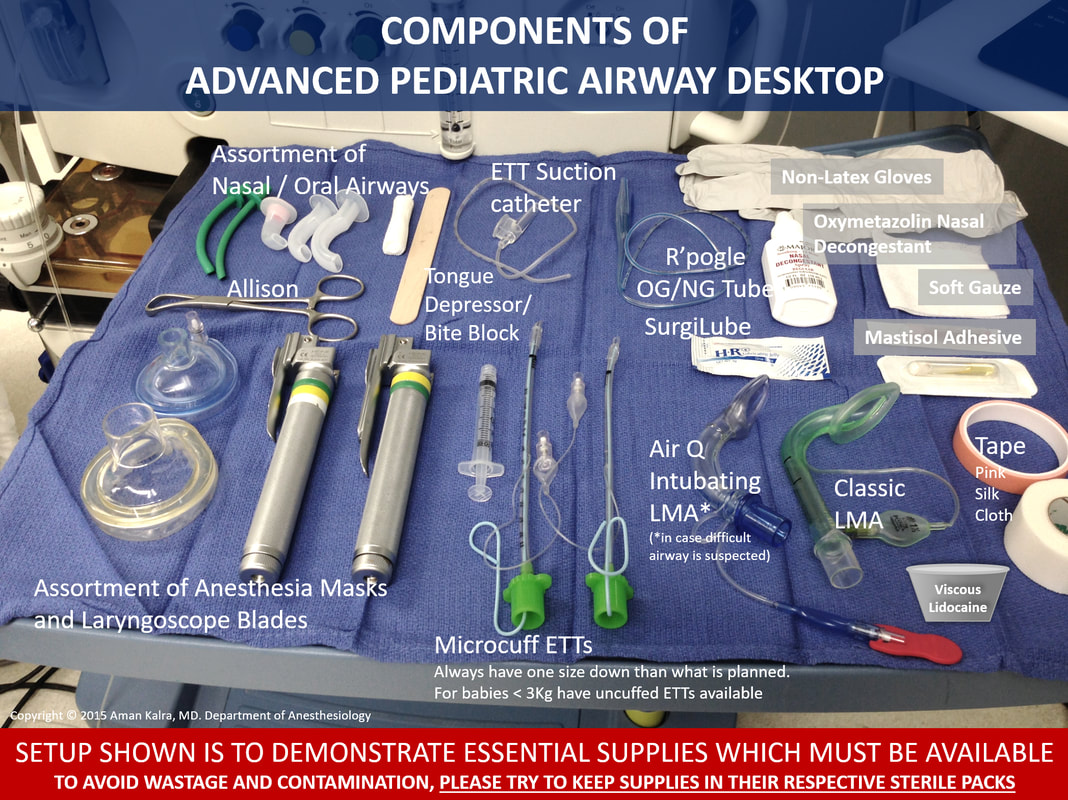
C. Components of Advanced Pediatric Airway Desktop Setup when Difficult Airway in Suspected or Known